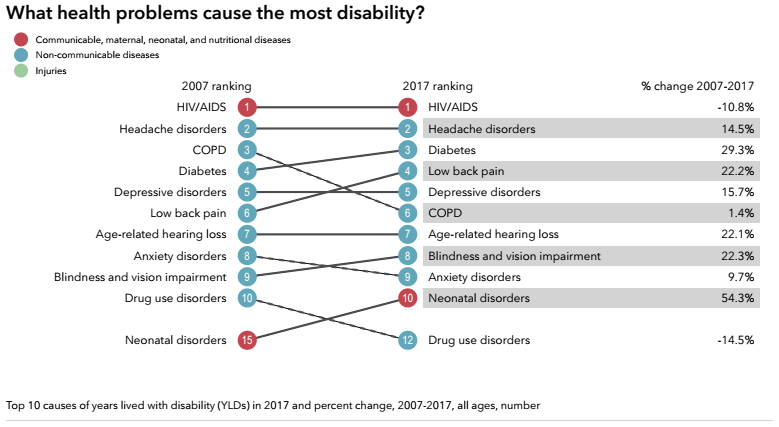
The leading cause of disablity in South Africa is hardly a surprise, HIV/AIDS. And, the good news is that there is a 10% reduction compared to 2007. But what this image shows is that NCDs (the blue dots) remain the largest group illnesses to cause disability irrespective of age. What is alarming is the for 6/8 NCDs listed, the increases are in double digits.
Disability measure =YLD
Disability is measured as by the amount of time, in years,that people lose to diseases and injuries = years of life lost to disability (YLD). A disabling condition does kill you but takes its personal and societal toll.
Calculating YLD
Mulitipy a disability’s severity by the time it lasts. This means that a short-term, severe health problem and a long-term, relatively mild health problem could both result in the same number of YLDs. For example, someone who needs two months to recover from a car accident but then regains their full health and someone who experiences relatively mild but lifelong back pain could end up losing the same number of years of their lives to disability. YLDs take into account all disabilities, including lower-visibility ones that result in daily pain, lost work time, or an inability for someone to thrive as they otherwise might.
Summary: 1st WHO essential diagnostic list focusing on mainly communicable diseases with a recommendation to include more NCDs in a future edition. PHC and facility level essential package. Vicki Pinkney-Atkinson
Improving NCDs diagnosis & treatment outcomes
Today, many people are unable to get tested for diseases because they cannot access diagnostic services. Many are incorrectly diagnosed. As a result, they do not receive the treatment they need and, in some cases, may actually receive the wrong treatment.
For example, an estimated 46% of adults with Type 2 diabetes worldwide are undiagnosed, risking serious health complications and higher health costs. Late diagnosis of infectious diseases such as HIV and TB increases the risk of spread and makes them more difficult to treat.
Essential Diagnostics List (EDL)
To address this gap, WHO today published its first Essential Diagnostics List (EDL), a catalogue of the tests needed to diagnose the most common conditions as well as a number of global priority diseases.
“An accurate diagnosis is the first step to getting effective treatment ….No one should suffer or die because of a lack of diagnostic services, or because the right tests were not available.”
Dr Tedros Adhanom Ghebreyesus, WHO Director-General.
The list concentrates on in vitro tests – i.e. tests of human specimens like blood and urine. It contains 113 products: 58 tests are listed for detection and diagnosis of a wide range of common conditions, providing an essential package that can form the basis for screening and management of patients. The remaining 55 tests are designed for the detection, diagnosis and monitoring of “priority” diseases such as HIV, TB, malaria, hepatitis B and C, human papillomavirus and syphilis.
Some of the tests are particularly suitable for PHC facilities, where laboratory services are often poorly resourced and sometimes non-existent; for example, tests that can rapidly diagnose a child for acute malaria or glucometers to test diabetes. These tests do not require electricity or trained personnel. Other tests are more sophisticated and therefore intended for larger medical facilities.
“Our aim is to provide a tool that can be useful to all countries, to test and treat better, but also to use health funds more efficiently by concentrating on the truly essential tests,” says Mariângela Simão, WHO Assistant Director-General for Access to Medicines, Vaccines and Pharmaceuticals. “Our other goal is to signal to countries and developers that the tests in the list must be of good quality, safe and affordable.”
For each category of test, the EDL specifies the type of test and intended use, format, and if appropriate for primary health care or for health facilities with laboratories. The list also provides links to WHO Guidelines or publications and, when available, to prequalified products.
Similar to the WHO Essential Medicines List, which has been in use for four decades, the EDL is intended to serve as a reference for countries to update or develop their own list of essential diagnostics. In order to truly benefit patients, national governments will need to ensure appropriate and quality-assured supplies, training of healthcare workers and safe use. To that end, WHO will provide support to countries as they adapt the list to the local context.
The EDL was developed following an extensive consultation within WHO and externally. The draft list was then considered for review by WHO’s Strategic Advisory Group of Experts on In-Vitro Diagnostics – a group of 19 experts with global representation. For more information see WHO website.
WHO will update the Essential Diagnostics List on a regular basis. In the coming months, WHO will issue a call for applications to add categories to the next edition. The list will expand significantly over the next few years, as it incorporates other important areas including antimicrobial resistance, emerging pathogens, neglected tropical diseases and additional NCDs.
RPN (ICU) Diabetes Nurse Specialist
SA NCD Alliance (SANCDA) Associate and Diabetes Education Society of South Africa (DESSA) member
Ramadan is approaching and people living with diabetes are advised to plan before starting the month-long fast. Approximately 100 million people with diabetes world-wide fast during Ramadan and most are able to fast the whole month. But this takes planning by all involved, including families, communities and health professionals.
What is Ramadan?
Ramadan is the ninth Islamic month and fasting during the day light hours is one of the five pillars of Islam. Muslims have been fasting during Ramadan for over 1400 years as prescribed in the Qur’an. Fasting is one part of the religious practices during Ramadan and adults must abstain from eating, drinking, sexual intercourse, use of oral medications, and smoking from before the sunrise to after sunset. There are no restrictions on food or fluid intake between sunset and dawn, however moderation is prescribed.
Most people consume two meals per day during Ramadan: one after sunset (referred to in Arabic as iftar or breaking of the fast meal), and the other before dawn of suhur (predawn).
When is Ramadan?
It varies according to the Muslim (lunar) calendar. This year it is approximately May 15th to June 14th 2018.
What are the diabetes numbers?
Over 425 million people worldwide live with diabetes
1 out of 2 adults with diabetes are undiagnosed.
About 80% of the world’s population live in low- and middle-income countries, like South Africa, where the greatest increase in diabetes will occur.
Diabetes is the #1 cause of death of females and the #2 cause of death for all in South Africa.
Muslims comprise almost ¼ of the world population and there are 148 million Muslims living with diabetes.
The International Diabetes Federation (IDF) projects that by 2045 the number of people living with the disease will more than double in the Middle East, Africa and South East Asia where the largest populations of Muslims live.
How does fasting affect people living with diabetes?
In people with diabetes the control of blood glucose needs more attention. Complications like low blood sugar (hypoglycaemia) and high blood glucose (hyperglycaemia), dehydration, and blood clots may occur. These are considered to be the “risks” of fasting and are potentially life threatening and require planning to avoid them such as changes to medication.
Preparation pre-Ramadan is essential and should include risk stratification. All planning must include education, nutrition, exercise, medication adjustments and monitoring. Ideally this should take place 6 – 8 weeks before Ramadan.
What about fasting when one takes medication for diabetes?
Islam does not burden its followers, there are exceptions for those who are unable to observe the obligatory fast. It is forbidden in Islam to exert oneself in any act that will bring harm upon oneself. Thus, if one is ill and the illness would be aggravated, or the pain would increase through fasting, then fasting is not required.
Those who do fast, are required to review their medication together with a health care practitioner and diabetes nurse specialist before Ramadan so adjustments can be made. In the event of any hypoglycaemia, the fast should be broken immediately and it is advised that the person should not resume fasting until a they consult a health care practitioner..
Who is a high risk during Ramadan?
Risk is assessed according to the following factors: type of diabetes, medication, previous Ramadan experience, hypoglycaemic risk, current complications, co-morbidities and individual work and/or social circumstances. Examples are old age with ill health, vascular complications, pregnancy and those doing intense physical labour.
What can be done to manage those at high risk of having complications?
Very high risk and high-risk patients should not fast. However, many will fast and these persons should be given the education on how to minimise the possible complications while fasting and thereafter. They should also be given an individualised management plan for reducing their risk for further complications.
The management plan should include pre-Ramadan visits, regular self-blood glucose monitoring before, during and after fasting, and a nutrition and exercise plan.
The plan must be individualised and tailored to the person’s circumstances, there is no “one size fits all.”
It is important to provide additional support to include emergency contacts and availability of a trained health care professionals in diabetes management at all times.
Include religious and community leaders, families and community members in the successful and uneventful fasting period.
Where can people find more information about diabetes and Ramadan?
Guidelines on the management of diabetes in Ramadan published in 2016 by the IDF Diabetes and Ramadan Alliance. These guidelines assist health care professionals and persons living with diabetes on the best practices in the preparation and treatment of those who will be fasting.
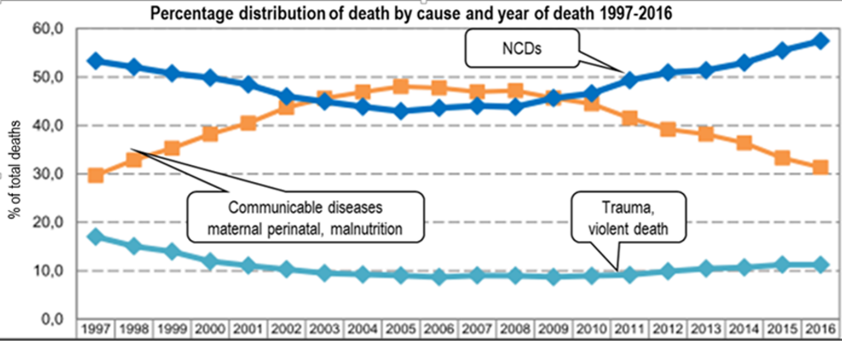
NCDs accounted for 57.4% of deaths in 2016 while communicable diseases were responsible for 31,3% of deaths. According to StatisticsSA this confirms that South Africa is in the midst of epidemiological change.
Each week we will be highlighting a story from the NCD Alliance’s Our Views Our Voices campaign. This week is the story of Rakiya from Nigeria, a woman living with Type 2 Diabetes and Arthritis this is her story.
Our Views, Our Voices
Our Views, Our Voices is an initiative that seeks to meaningfully involve people living with NCDs in the NCD response, supporting and enabling individuals to share their views to take action and drive change.
Our Views, Our Voices is a five-year initiative (2016-2020) built around four main pillars of work: consultation, campaigns, communications, and capacity development.